
It's Time to Retire 3.3 million: A Modern Estimate of the U.S. Skin Cancer Burden
Dermatology has quoted the same nonmelanoma skin cancer numbers for fourteen years. The population they describe no longer exists.
For more than a decade, nearly every conversation about the scale of skin cancer in the United States has opened the same way: roughly 5.4 million cases of nonmelanoma skin cancer (NMSC) are treated each year in about 3.3 million Americans. Those figures appear in patient brochures, society fact sheets, payer policies, investor decks, and the introduction of seemingly every NMSC research paper published since.
They come from a single, excellent source — Rogers and colleagues, writing in JAMA Dermatology in 2015. But that study described the year 2012. We are now in 2026. The 3.3 million figure is fourteen years old, and the authors themselves did not present it as a fixed number. They presented it as a point on a steep upward curve, explicitly documenting “continued increases” in both diagnoses and affected patients.
The field has frozen a moving number. It is time to thaw it.
First, get the units right
Before proposing a new figure, it is worth correcting an error that has crept into the way these numbers are repeated. The 5.4 million and the 3.3 million are not interchangeable, and they are not the same kind of thing:
5.4 million is the estimated number of cancers (lesions) treated.
3.3 million is the estimated number of people treated.
The 2012 study found roughly 1.43 treated lesions per affected patient. Any modern estimate must honor that distinction, and report both numbers, or it will be rightly picked apart. Throughout this piece, “incidence” refers to affected people unless a lesion count is specified.
A defensible 2026 estimate: 4.7 million people
We propose that the dermatologic community adopt a working estimate of approximately 4.7 million Americans diagnosed with NMSC annually, corresponding to roughly 6.7 to 7.7 million lesions (applying the established 1.43–1.63 lesions-per-person ratio).
This is not an aggressive number. It is a conservative one. Here is why, built from the ground up using several independent methods that converge.
Method one — demographics alone, with risk frozen at 2012 levels. NMSC is overwhelmingly a disease of older adults; roughly 80% of cases occur in people aged 60 and over. The 65-and-older U.S. population has grown from 43.1 million in 2012 to roughly 64 million in 2026 — an increase of nearly 50% (U.S. Census Bureau; Population Reference Bureau). If we take the 2012 base of 3.3 million people, assign 80% to the older cohort and grow it with that cohort, and grow the remaining 20% with the general adult population, we arrive at approximately 4.7 million, assuming no increase in per-person risk. In other words, 4.7 million is roughly what the aging of America produces by itself, before counting a single additional point of rising incidence.
Method two — conservative compound growth. Between 2006 and 2012, the number of affected people grew at about 7% per year, and the age-adjusted incidence rate itself climbed from 6,075 to 7,320 per 100,000. No one should extrapolate 7% indefinitely but apply just one-third of that historical rate, roughly 2.5% per year, from 2012 to 2026, and the result is again approximately 4.7 million.
Method three — independent survey corroboration. A separate methodology, the Medical Expenditure Panel Survey analyzed by Guy and colleagues (American Journal of Preventive Medicine, 2015), found that the number of U.S. adults treated for NMSC rose from 3.1 million in 2002 to 4.3 million in 2011. That figure had already crossed four million more than a decade ago, by a completely different counting method. Against that backdrop, 4.7 million in 2026 is, if anything, on the low side.
Method four — the upper bound. Extending the 2006–2012 trend in a straight line would put 2026 closer to 5.9 million people. We do not advocate that figure; we cite it to show where the conservative end of the honest range sits.
Two independent methods land on 4.7 million as a floor, and the others sit above it. That convergence, not any single calculation, is the case for the number.
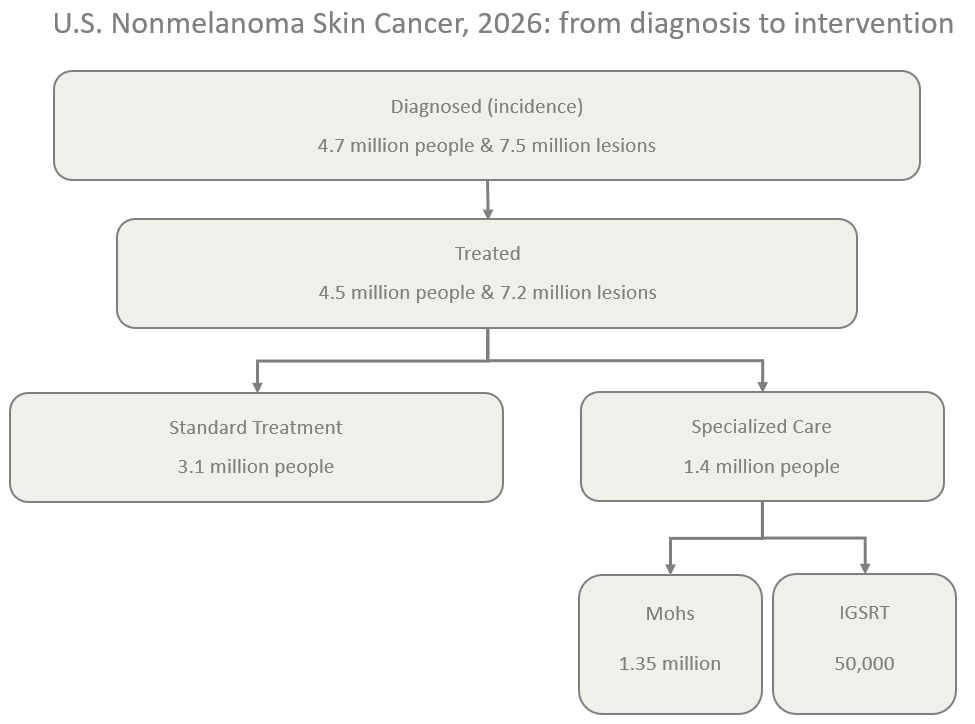
From diagnosis to intervention: the funnel
A modern estimate should not stop at incidence. The more useful question for clinicians, payers, and patients is what happens after diagnosis. Not everyone diagnosed is treated, and among those treated, the intensity of intervention varies enormously.
Diagnosed: ~4.7 million people / ~6.7–7.7 million lesions.
Treated: ~4.5 million people / ~6.4–7.3 million lesions. Long-term cohort data indicate that roughly 3% of diagnosed NMSC receives no active treatment, managed by observation, topical agents, or removed by the diagnostic biopsy itself. That places active treatment at about 96% of diagnoses.
Standard treatment: ~3.1 million people. The majority of treated cases are addressed with office-based destruction (electrodesiccation and curettage, cryotherapy), simple surgical excision, or topical therapy. For many small, low-risk, well-defined tumors, this is appropriate and curative.
Specialized intervention: ~1.4 million people / ~1.6 million lesions. A substantial minority of cases, high-risk sites, aggressive histologies, recurrent or large tumors, and patients who are poor surgical candidates, call for margin-controlled or precision modalities: Mohs micrographic surgery and image-guided superficial radiation therapy (IGSRT).
Within that specialized tier, Mohs is the dominant modality. Medicare Mohs case volume rose from 558,447 in 2009 to 700,262 in 2013, and first-stage Mohs billing reached 816,455 by 2019 while growing roughly 5% per year. Because that data captures only Original Medicare and excludes Medicare Advantage, now about half of all Medicare, plus commercial and under-65 cases, national Mohs volume is on the order of 1.5 million cases per year and rising.
The bottleneck and where IGSRT fits
Demand for specialized NMSC intervention is rising in lockstep with incidence, but the supply of the dominant modality is capped. Mohs is a fellowship-trained discipline; the adequacy of the Mohs surgeon workforce is an openly acknowledged concern, and board eligibility is tightening to fellowship-trained physicians. You cannot scale 1.4 million specialized cases a year in a workforce that grows slowly by design and centralizes around larger metropolitan areas.
This is the gap that image-guided superficial radiation therapy is positioned to help fill. IGSRT, superficial radiation paired with high-resolution dermal ultrasound, was FDA-cleared in 2015 and has demonstrated cure rates above 99% in early-stage BCC, SCC, and SCC in situ, with outcomes in published series comparable to Mohs and a favorable toxicity profile for patients who wish to avoid or cannot undergo surgery.
We want to be precise, and deliberately modest, about IGSRT’s current scale. GentleCure by SkinCure Oncology, which is responsible for at least 90% of all IGSRT treatments in the United States and tracks every one of those treatments, projects approximately 45,000 patients (about 72,000 lesions) in 2026. That implies national IGSRT volume of roughly 50,000 patients — about 1% of all treated NMSC, and a small fraction of the specialized tier.
The number that matters is not the snapshot, but the slope. GentleCure’s IGSRT volume has grown from 1,521 patients in 2017 to a projected 45,000 in 2026 — roughly a thirty-fold increase, settling into steady growth of about 28% per year. Cumulatively, that’s 150,000 patients treated with GentleCure, or 180,000 patients treated with IGSRT, the largest real-world IGSRT evidence base in existence. A modality at 1% of the market, compounding at nearly 30% a year, against a specialized-care tier that is growing while its dominant modality cannot is the trajectory worth watching.
The ask
We are not necessarily asking the field to adopt our company’s numbers. We are asking it to stop citing a number from 2012.
Specifically:
Retire “3.3 million” and “5.4 million” as present-tense statistics. They describe a country that has since added 20 million people over the age of 65.
Adopt a modern working estimate — we propose 4.7 million people and 6.7–7.7 million lesions. Label it as an estimate, with its methodology and uncertainty stated plainly.
Distinguish diagnosis from treatment from intensity of intervention. A single headline number obscures the part of the burden that is growing fastest and straining hardest against capacity.
Fund a proper re-estimate. The reason the field still leans on 2012 is that NMSC is not captured in national cancer registries. That is a solvable problem, and the organizations that benefit from accurate numbers should help solve it.
It’s fairly absurd that a company that treats skin cancer should be the one calling for a more honest count of it, but someone must move first. The patients behind these numbers, and there are far more of them than we have been saying, deserve a field that counts them as they are today, not as they were fourteen years ago.
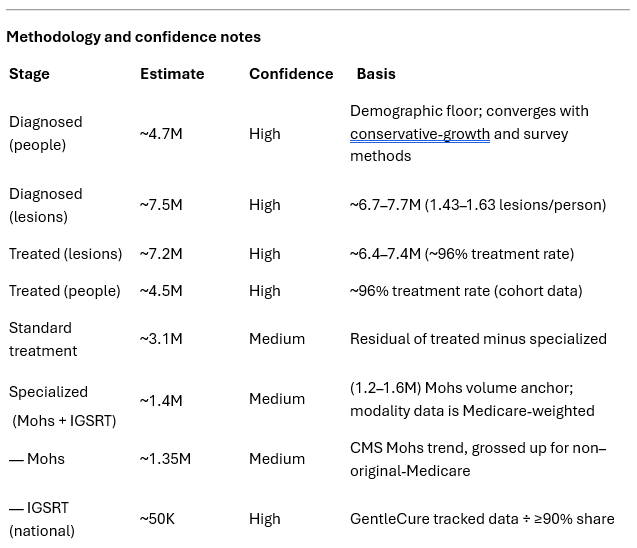
Note on the specialized tier: This is the softest figure in the model, because published modality splits skew toward Mohs (drawn from elderly, Medicare, and academic samples). It should be presented as a range. The IGSRT figure, by contrast, is the one number in the entire funnel that is measured rather than modeled.
Primary sources: Rogers HW et al. JAMA Dermatol. 2015;151(10):1081–1086 (and Arch Dermatol. 2010 for 2006). Guy GP Jr et al. Am J Prev Med. 2015;48(2):183–187 (MEPS). U.S. Census Bureau / Population Reference Bureau (65+ population). CMS Medicare Mohs utilization data (Kantor; Johnstone et al.; CPT 17311 billing analyses). IGSRT clinical literature (Oncology and Therapy, 2024; JAAD-indexed cohort studies). GentleCure / SkinCure Oncology internal treatment data, 2017–2026