
The Most Common Cancer We Don't Count
Why there is no nonmelanoma skin cancer registry — and why it's time to build one
Every day in the United States, roughly 9,500 people are diagnosed with skin cancer. The overwhelming majority have nonmelanoma skin cancer (NMSC), basal cell carcinoma or squamous cell carcinoma, the most common malignancy in the country and, by most estimates, in the world.
And yet, if you went looking for an authoritative national count of how many people developed NMSC last year, you would not find one. The most-cited figure — roughly 5.4 million cases treated in about 3.3 million people — comes from an analysis of data from 2012. More than a decade later, it remains the number researchers, clinicians, and advocates reach for, not because it is current, but because there is nothing newer to cite.
This is the quiet paradox at the heart of skin cancer epidemiology: the cancer we see most is the cancer we measure least. To understand why that gap exists and why it matters more than it might first appear, it helps to start with the often-invisible infrastructure that makes cancer statistics possible in the first place.
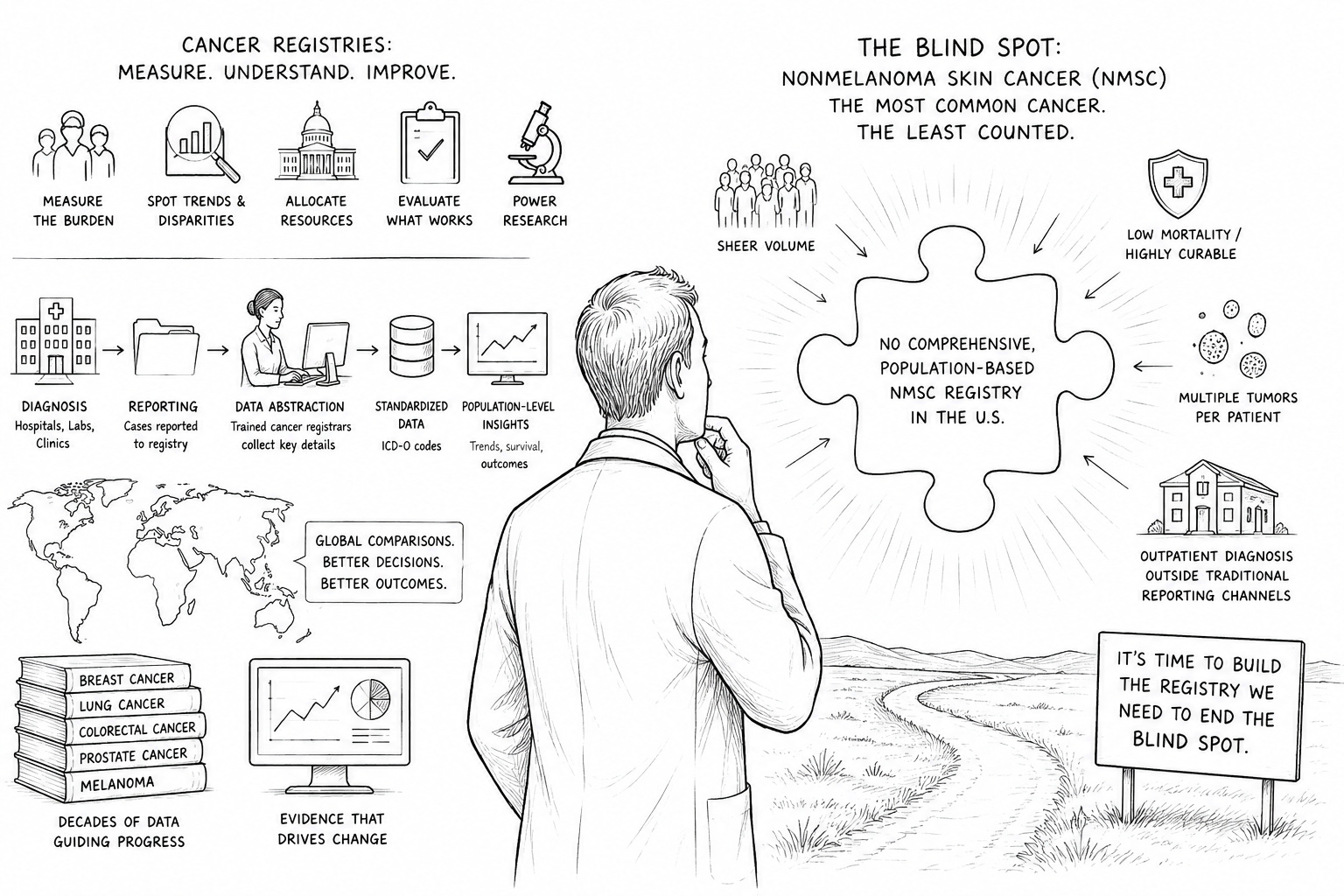
What is a cancer registry?
A cancer registry is a systematic system for collecting, storing, and analyzing data about people diagnosed with cancer. At its simplest, it answers a deceptively important question: who is getting cancer, where, when, and what happens to them next?
There are two broad types. Hospital-based registries track patients treated within a single institution or health system, supporting quality improvement and follow-up care. Population-based registries are the more powerful tool: they aim to capture every cancer case occurring in a defined geographic population, regardless of where the person is treated. It is population-based registries that produce the incidence rates, survival statistics, and trend lines that shape public health.
In the U.S., two programs anchor this work: the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) program and the CDC’s National Program of Cancer Registries (NPCR). Internationally, the International Agency for Research on Cancer (IARC) coordinates registries across dozens of countries, enabling global comparisons. Together, these systems form one of the most valuable scientific assets in all of medicine.
How registries actually work
A registry is essentially a structured pipeline. When a cancer is diagnosed, typically confirmed by a pathologist examining tissue, the case is reported to the registry by hospitals, laboratories, treatment centers, and physicians. Trained cancer registrars then abstract the relevant details: tumor type and location, stage at diagnosis, the patient’s demographics, the treatments delivered, and, over time, outcomes such as recurrence and survival.
To make this data comparable across institutions and borders, everything is translated into standardized codes, most notably the International Classification of Diseases for Oncology (ICD-O). Standardization is what allows a researcher to compare melanoma incidence in Connecticut with melanoma incidence in Queensland, or to track whether a cancer’s rate is genuinely rising or merely being detected more often.
The result is a longitudinal, population-level picture of a disease that no single hospital, insurer, or clinician could ever assemble alone.
Why registries matter
Registries are not a bureaucratic formality. They are the empirical foundation on which modern cancer control is built. Reliable registry data makes it possible to:
Measure the true burden of a disease — how many people are affected, and whether that number is climbing or falling.
Spot trends and disparities — geographic clusters, demographic gaps, and inequities in who gets diagnosed early versus late.
Allocate resources rationally — directing screening programs, funding, and clinical capacity to where the need is greatest.
Evaluate what works — measuring whether new treatments and prevention efforts actually change outcomes at the population level.
Power research and clinical trials — providing the denominators and comparison groups that turn anecdotes into evidence.
Put simply: you cannot manage what you do not measure. For most major cancers — breast, lung, colorectal, prostate, melanoma — we have decades of registry data telling us exactly where we stand. For the single most common cancer of all, we do not.
The blind spot: why there is no NMSC registry
Here is the part that surprises almost everyone who learns it. In the United States, basal cell and squamous cell carcinomas of the skin are explicitly excluded from the major cancer registries. Per the CDC, NPCR- and SEER-supported registries report essentially all malignant cancers with the exception of basal and squamous cell carcinomas of the skin (the lone carve-out being those occurring on genital skin). Reporting NMSC is, quite simply, not required.
This was not an oversight. It was a series of practical decisions, each defensible on its own terms:
Sheer volume. NMSC dwarfs every other cancer in frequency. Capturing every basal cell carcinoma would impose an enormous reporting burden on a system designed around comparatively rarer, more lethal cancers.
Low mortality. Because NMSC is usually highly curable, registries historically prioritized cancers that kill more often.
Multiple tumors per patient. It is common for one person to develop many separate NMSC lesions over a lifetime, and registries lack consistent rules for how to count them.
Outpatient diagnosis. Increasingly, NMSC is diagnosed and treated in dermatology offices and other outpatient settings that fall outside the traditional hospital-and-laboratory reporting channels registries were built around.
The cumulative effect is that there is no comprehensive, population-based incidence registry for the most common cancer in the world. What estimates we do have are stitched together from Medicare claims, survey data, and special studies, all useful but indirect and quickly outdated. A handful of narrow, disease-specific or treatment-outcome registries exist, but none provides the population-level surveillance that defines a true cancer registry.
The cost of not counting
It is tempting to shrug this off. If NMSC is so curable, does precise counting really matter? It does — for reasons that compound over time.
First, we are effectively flying blind on a moving target. The diagnosis and treatment of NMSC in the U.S. increased by an estimated 77% between 1994 and 2014, and incidence has continued to climb with an aging population and cumulative sun exposure. Without current data, we cannot say with confidence how fast the burden is growing, where, or in whom.
Second, the human and economic stakes are real. Skin cancer is by far the most frequently diagnosed cancer in the U.S. More Americans are diagnosed with it each year than with all other cancers combined, and roughly one in five Americans will develop it by age 70. Treating NMSC costs an estimated several billion dollars annually. And while individual cases are rarely fatal, the disease is far from harmless: worldwide, thousands of people die of nonmelanoma skin cancer every month, and aggressive squamous cell carcinomas can metastasize. A cancer this prevalent deserves the same epidemiological seriousness we extend to every other.
Third, the data gap distorts everything downstream. Without robust registry data, we cannot reliably measure disparities in access and outcomes, compare the long-term effectiveness of different treatment approaches at scale, identify geographic or occupational risk patterns, or properly inform prevention and screening policy. Researchers studying NMSC are forced to validate their work against proxies rather than a gold-standard population dataset, and that’s a structural handicap that slows progress across the entire field.
We have, in other words, built a sophisticated measurement system for cancer and then pointed it away from the cancer that affects the most people.
The case for building one
A dedicated NMSC registry — ideally population-based and, eventually, international — would close that gap. It would give us, for the first time, an accurate and current picture of the world’s most common cancer: how many people it affects, how that is changing, who bears the greatest burden, and which interventions genuinely improve outcomes.
The objections that justified excluding NMSC decades ago are increasingly answerable. Electronic health records, structured pathology reporting, natural-language processing, and modern data infrastructure make large-scale capture far more feasible than it was when these decisions were originally made. The volume that once made counting impractical is precisely what makes counting worthwhile.
A turning point in Geneva
There are encouraging signs that the field is ready to take this on. At the 2024 World Cancer Congress in Geneva, the biennial convening of the Union for International Cancer Control (UICC), leadership from GentleCure by SkinCure Oncology brought this exact argument to the global cancer-control community. CEO Kerwin Brandt and Chief Innovation Officer Steven Scott presented on “Redefining Skin Cancer: The Urgent Need for Innovation in Nonmelanoma Diagnosis and Treatment,” and a patient’s NMSC treatment story was featured in the UICC’s “Rewriting Cancer” series.
Crucially, those conversations extended to the data gap itself. In meeting with the UICC to discuss the development of a worldwide NMSC registry, GentleCure’s leadership found a receptive audience, with the UICC agreeing that such an effort would be a worthwhile endeavor. For a disease that has gone uncounted for decades, recognition at this level is a meaningful first step: an acknowledgment from the world’s leading cancer-control organization that the most common cancer should no longer be the least measured.
The path forward: a coalition to count the uncounted
Recognition is a beginning, not an end. A nonmelanoma skin cancer registry will not emerge from any single institution, because no one organization holds both the will to demand it and the means to build it. The will belongs to advocates and patients; the means belong to the agencies and clinicians who run cancer surveillance. Progress depends on bringing both to the same table.
A coalition equal to the task might include:
SkinCure Oncology, as a leader in the noninvasive treatment of NMSC, contributing clinical insight, treatment-outcome data, and a direct stake in measuring what actually works at scale.
The Skin Cancer Foundation, the leading voice in skin cancer advocacy and public education.
The American Cancer Society, a leading force in cancer advocacy broadly, with the convening power to elevate NMSC surveillance on the national agenda.
AARP, advocating for the older adults who shoulder the greatest share of the NMSC burden, a population too often left out of the conversation.
Advocacy alone, however, cannot create a registry. That requires the organizations that own the infrastructure: the National Cancer Institute’s SEER program and the CDC’s National Program of Cancer Registries in the United States, and the International Agency for Research on Cancer and the UICC internationally. Just as important, because a registry is only ever as complete as the reporting that feeds it, the clinicians who diagnose NMSC every day, dermatologists, Mohs surgeons, and the pathologists who confirm these cancers, must be partners from the outset, not afterthoughts.
The pieces already exist. What has been missing is the shared resolve to assemble them. The 2024 World Cancer Congress suggested that resolve is now within reach.
What gets counted, counts
Cancer registries are among the most important tools we have ever built for understanding and ultimately defeating cancer. They turned scattered case reports into trend lines, survival curves, and disparities maps that drive prevention, funding, and research. For nearly every major cancer, that infrastructure exists.
Nonmelanoma skin cancer, the most common of them all, has been left out. The reasons made sense once. They make less sense now, in an era of digital health records and rising incidence, and they will make even less sense a decade from now if we continue to manage the world’s most common cancer using a number from 2012.
Building a nonmelanoma skin cancer registry is not a minor data-cleanup project. It is a statement about whose disease matters and what we are willing to measure. It is time to count the cancer we see the most.
What’s next?
Over the months ahead, the team at GentleCure by SkinCure Oncology intends to keep this conversation moving — among the researchers, advocates, clinicians, and policymakers who share an interest in building a national NMSC registry.
In the meantime, we’re done citing a 14-year-old estimate as the definitive measure of how many Americans develop NMSC each year. Using the data already available and a transparent, common-sense methodology, we’ve developed a new projection of the disease’s true incidence, and in the weeks ahead, we’ll share both the numbers and exactly how we arrived at them.
A registry remains the goal. But better counting doesn’t have to wait for one.
The Skin Cancer Treatment Journal explores advances in the understanding and treatment of skin cancer.
Sources & further reading
CDC, U.S. Cancer Statistics — Cautionary Notes (NPCR/SEER reporting exclusions): https://www.cdc.gov/united-states-cancer-statistics/public-use/cautionary-notes.html
CDC, U.S. Cancer Statistics — Incidence Data Sources: https://www.cdc.gov/united-states-cancer-statistics/technical-notes/incidence-data-sources.html
Skin Cancer Foundation, Skin Cancer Facts & Statistics: https://www.skincancer.org/skin-cancer-information/skin-cancer-facts/
American Cancer Society, Basal & Squamous Cell Skin Cancer Key Statistics: https://www.cancer.org/cancer/types/basal-and-squamous-cell-skin-cancer/about/key-statistics.html
U.S. Preventive Services Task Force evidence review (keratinocyte carcinoma not reportable): https://www.ncbi.nlm.nih.gov/books/NBK591450/
The Surgeon General’s Call to Action to Prevent Skin Cancer: https://www.ncbi.nlm.nih.gov/books/NBK247164/
“A Narrative Review of European Registries for Skin Cancer” (NMSC under-registration): https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12896798/
SkinCure Oncology at the 2024 World Cancer Congress, Geneva: https://www.prnewswire.com/news-releases/skincure-oncology-executives-address-world-cancer-congress-in-geneva-celebrate-patient-video-about-treating-common-skin-cancer-with-image-guided-srt-302260249.html
Union for International Cancer Control, World Cancer Congress: https://www.uicc.org/what-we-do/events/world-cancer-congress