
The Truth Behind Neglected Tumors
Identifying and Removing the Barriers Between Diagnosis and Treatment
As a child of the 1980s who spent part of my early years living in St. Croix, I grew up under the Caribbean sun long before we fully understood the long-term consequences of ultraviolet exposure. Today, I am a skin cancer survivor myself.
I have also spent nearly two decades as a healthcare leader caring for patients and the clinical team responsible for patient care. Those experiences have given me a particular vantage point. One that lets me understand both the patient sitting in the exam room and the healthcare system surrounding them.
From the outside, the decision seems simple. When most people hear the words skin cancer, they assume the next step is obvious: get it treated.
But that’s not always what happens.
Every year, millions of Americans are diagnosed with nonmelanoma skin cancer (NMSC), primarily basal cell carcinoma (BCC) and squamous cell carcinoma (SCC). Many of these patients see a suspicious spot, visit a dermatologist, undergo a biopsy, and receive a definitive diagnosis. Yet a surprising number never move forward with treatment, or they delay it for months or even years.
Why?
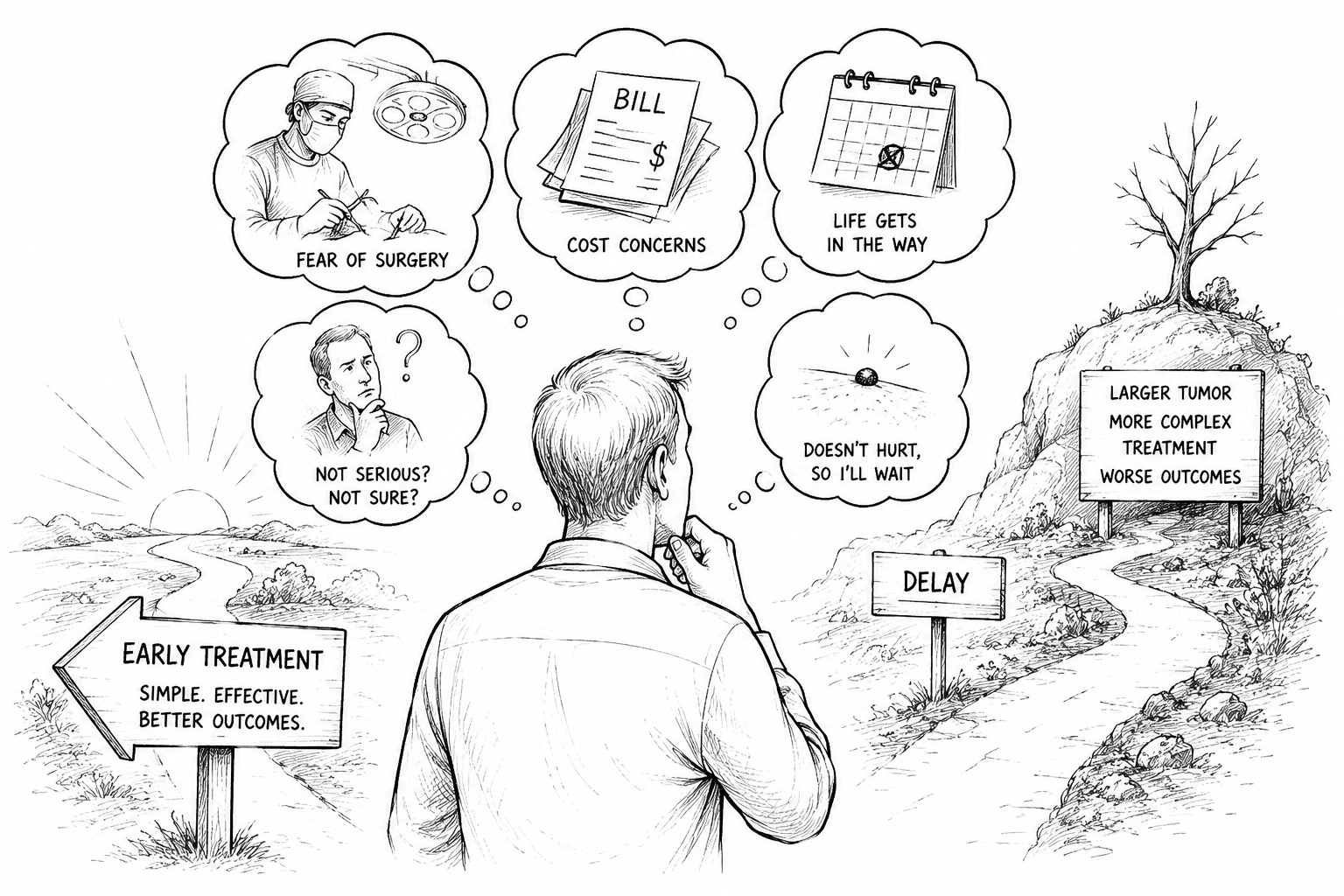
Over the years, I have become increasingly convinced that most untreated skin cancers are not the result of negligence. More often, they are the result of barriers that stand between a diagnosis and a patient’s ability or willingness to act on it. Those barriers tend to fall into a handful of recurring categories: misunderstanding of risk, fear of treatment, financial and time pressure, limited access to care, the weight of prior treatment experiences, and competing life priorities.
In my experience, most patients want treatment. What they need is a pathway that is accessible, understandable, and aligned with their individual circumstances. We often assume that once a diagnosis is made, treatment naturally follows. The reality is far more complicated, because patients do not experience a diagnosis in isolation. They experience it through the lens of their finances, their families, their geography, their previous encounters with the healthcare system, and their fears.
Understanding those barriers may be one of the most important opportunities we have to improve outcomes for patients facing skin cancer.
“It’s Just Skin Cancer”: The Risk Patients Underestimate
One of the greatest challenges in skin cancer care is that nonmelanoma skin cancers often do not look or feel dangerous.
Unlike many other cancers, a basal cell carcinoma may grow slowly. It may not hurt. It may not interfere with daily life. In some cases, patients live with a lesion for years before seeking treatment. This creates a false sense of security.
The asymptomatic nature of these tumors compounds the problem. Human nature prioritizes urgent problems: a painful tooth gets attention, chest pain gets attention. A spot on the skin that doesn’t hurt often falls to the bottom of the list. But cancer biology does not depend on whether a lesion is painful. Many neglected tumors begin as small, asymptomatic lesions that gradually enlarge over time, and by the time symptoms appear, treatment can become more complicated and the cosmetic consequences more significant.
Because NMSC is rarely discussed in the same terms as breast, lung, or melanoma, many patients underestimate its potential. Yet untreated tumors can continue to grow, invade surrounding tissue, and eventually require larger, more complex procedures to remove. Delayed treatment has been associated with continued tumor growth and increasing treatment complexity.1,7
The irony is that the earlier a skin cancer is treated, the simpler treatment often becomes. As I often say: early diagnosis, good prognosis.
The Fear of Treatment
For many patients, the word cancer is frightening. But for others, the proposed treatment is more intimidating than the diagnosis.
A patient who hears they need surgery on their nose, ear, cheek, scalp, or lower leg may immediately imagine pain, stitches, scarring, healing time, changes in appearance, or additional reconstructive procedures. Research into why patients fail to proceed with recommended treatment has identified treatment-related concerns as a significant factor in non-adherence.2
These fears are understandable. As a skin cancer survivor myself, I understand them personally.
And for many patients, the concern extends beyond the procedure itself. Skin cancer frequently occurs on the most visible parts of the body—the nose, ears, lips, eyelids, scalp, and face. Patients naturally worry about scarring, tissue loss, reconstruction, and how treatment may affect their appearance or sense of identity.
These concerns should not be dismissed as vanity. Appearance influences confidence, social engagement, and emotional well-being. A patient weighing treatment on the center of their face is often contemplating far more than a clinical outcome. They are thinking about how they will look to their spouse, their grandchildren, their coworkers, and themselves. When providers acknowledge these concerns rather than minimize them, trust tends to increase and treatment conversations become more productive.
What patients may not realize is that treatment options have evolved. Surgery remains an important and effective treatment for many skin cancers, but in appropriate cases it is no longer the only option. Advances in both surgical and non-surgical therapies have expanded what is available to patients and when patients understand they may have choices, the conversation often changes.
When Patients Grow Tired of Being Treated
A group too often overlooked are patients who have already undergone numerous procedures.
Dermatologists routinely care for patients who have accumulated multiple skin cancers over a lifetime with repeated excisions, Mohs surgeries, grafts, flaps, and reconstructions. Many remain highly satisfied with their care. But repeated treatment can create what some clinicians informally call treatment fatigue.
These patients are not refusing care. They are seeking a different experience of it. The prospect of another procedure, another recovery, another bandage can become emotionally exhausting over time. Previous treatment experiences frequently shape future treatment decisions, which is why meeting patients where they are, rather than where we assume they should be, matters so much.
The Psychological Weight of Skin Cancer
Skin cancer is often called the “good cancer,” or “just skin cancer.” Usually intended to reassure, those phrases can unintentionally minimize the emotional burden of a cancer diagnosis.
A growing body of research shows that skin cancer can affect psychological well-being, body image, anxiety, and overall quality of life. Patients may worry about recurrence. They may fear disfigurement. They may relive a difficult prior experience, or grow anxious every time they notice a change in their skin. For those who have been through multiple procedures, these emotions accumulate.
This matters because what looks like procrastination is often something else entirely—fear, anxiety, or emotional exhaustion. Recognizing that distinction allows providers to support patients rather than judge them, and to remove the barriers that quietly delay timely treatment.
The Cost and Time Question
Healthcare decisions are rarely made in a vacuum.
Even insured patients worry about deductibles, copays, transportation, lost work time, and caregiving responsibilities. For retirees on fixed incomes, an unexpected medical expense can feel overwhelming. For working adults, multiple office visits can collide with employment and family obligations.
Patients don’t always voice these concerns to their physicians. Instead, they postpone treatment, intending to address it later. Unfortunately, later can become months—or years. Financial and time toxicity are increasingly recognized as factors in healthcare decisions across many conditions, and skin cancer is no exception.
Further, the payor system is quick to lag (self-interest lag) in payment and medical policies for advanced, modern techniques, forcing higher out-of-pocket consequences to the patients. A different subject, but one I attend to expand on…
Access Is Not Equal
We often assume that once a diagnosis is made, treatment is readily available. For many Americans, that assumption is wrong.
Significant portions of the United States lack local access to specialty skin cancer care. Many rural communities have few dermatologists, Mohs surgeons, or radiation oncologists, requiring patients to travel substantial distances for consultation and treatment.4, 5, 6
For some patients, transportation is the barrier. For others, it’s time away from work or family. For elderly patients, it may be the loss of a spouse who once drove them to appointments, or the difficulty of navigating multiple visits alone.
Healthcare leaders tend to focus on treatment efficacy while overlooking treatment accessibility. Yet the most effective therapy in the world provides little benefit if a patient cannot realistically reach it. When we talk about neglected tumors, we have to recognize that some patients are not avoiding care. They are struggling to access it.
When Life Gets in the Way
Sometimes the reason has nothing to do with skin cancer at all.
A spouse becomes ill. A grandchild needs care. A patient is already managing heart disease, diabetes, or another serious condition. Studies of patients who chose watchful waiting or deferred treatment have shown that competing health priorities and limited life expectancy frequently shape these decisions.3
Some delays are entirely understandable. But many patients underestimate the cumulative effect of postponement. Skin cancer does not pause while life gets busy.
The Communication Gap
Perhaps the most important lesson is that patients do not always hear what providers believe they are saying.
A physician says, “This is a basal cell carcinoma.” The patient hears, “It’s not a serious cancer.”
A physician says, “We should remove this.” The patient hears, “I have plenty of time.”
A physician says, “This is a straightforward procedure.” The patient hears, “I’m going to lose part of my nose.”
The difference matters. Patients filter information through personal experience, fear, financial reality, family obligation, and prior encounters with the healthcare system. Effective communication requires more than delivering a diagnosis. It requires understanding the patient’s perspective and addressing the barriers that may stand between diagnosis and treatment.
Moving Beyond Fear
The goal should never be to pressure patients toward a particular treatment. After all, it is their story, not ours.
The goal is to empower them. Patients deserve clear information and transparency about risks, benefits, costs, expectations, and outcomes. Most of all, they deserve to understand the full range of treatment options that may be available to them. The objective is not to determine what every patient should do. It is to ensure patients know what they can do!
The truth behind neglected tumors is not that patients don’t care about their health. More often, they encounter barriers. Fear, access, cost, competing priorities, prior experience, or simple misunderstanding. Our responsibility as healthcare leaders is to identify and remove those barriers.
Because when patients are informed, empowered, and given access to care, they are far more likely to move forward. And when they move forward, outcomes improve.
In the end, the patient—and their story—is the point!
References
1 Alam M, Goldberg LH, Silapunt S, Gardner ES, Strom SS, Rademaker AW, Margolis DJ. Delayed treatment and continued growth of nonmelanoma skin cancer. Journal of the American Academy of Dermatology. 2011;64(5):839-848.
2 Cho SK, Li S, et al. Non-adherence of surgical treatment in patients with non-melanoma skin cancer. Dermatology. 2023.
3 van Winden MEC, Bastiaens MT, et al. Evaluation of watchful waiting and tumor behavior in patients with basal cell carcinoma. JAMA Dermatology. 2021;157(10):1174-1181.
4 Resneck JS Jr, Kimball AB. The dermatology workforce shortage. Journal of the American Academy of Dermatology. 2004;50(1):50-54.
5 Health Resources and Services Administration (HRSA). Health Professional Shortage Areas (HPSA) data and workforce reports. U.S. Department of Health and Human Services.
6 American Society for Radiation Oncology (ASTRO). Radiation oncology workforce and geographic access to care reports.
7 Eide MJ, Weinstock MA, Dufresne RG Jr, et al. Relationship of treatment delay with surgical defect size from keratinocyte carcinoma. Journal of Investigative Dermatology. 2005;124(2):308-314.
Josh Swindle is a skin cancer survivor and a healthcare leader who has spent nearly two decades working alongside physicians, therapists, and care teams focused on improving access to cancer treatment across the United States.
Disclosure: Josh Swindle is an executive at SkinCure Oncology. The views expressed here are his own.